

Blogs are opinion pieces and reflect their author’s views
Knowledge from the North: Research in Canada Underscores the Importance of the Social Determinants to Improve Population Health
Written by: Daniel J. Dutton and PG Forest
It may surprise some policy-makers to hear it, but the best way for government to use its financial resources to improve population health in a developed country is to spend more on social services rather than on health care.
Models using data from the United States, Canada, and across the 36 countries of the Organization for Economic Cooperation and Development (OECD) all show similar trends: a dollar spent on social services has a higher rate of return – compared to a dollar spent on health care – for achieving outcomes like longer life expectancy and lower mortality rates from preventable or treatable causes. Even deaths attributable to highly behavioral factors, such as diabetes or alcohol, appear to diminish as a consequence of more spending on social services.
In short, it is crystal clear that focusing more attention and resources on the Social Determinants of Health and Well-Being (colloquially, where we live, work and play) yields better outcomes in almost every way. Notwithstanding the evidence, however, health care spending dominates the way that the public and policymakers think about population health in most countries.
_________________________________________________________________
The Social Determinants of Health and Well-Being will be the subject of the second presentation in the Deeper Dive Webinar Series from the National Interoperability Collaborative (NIC). It’s titled “Knowledge from the North,” and will feature two of the Canadian researchers who conducted the study discussed in this blog, as well as other subject-matter experts. Learn more about the webinar and register here.
_____________________________________________________________________
In the years prior to enactment of the Affordable Care Act (ACA), a consensus emerged in the U.S. that escalating health care outlays were among the most serious policy challenges faced by the country’s government, businesses and families. Total health spending at the time had reached 17.3 percent of GDP, higher than in any other modern economy. Yet it was generally agreed that Americans did not receive great value back from their investment, considering the health status of the population and the difficulty of assuring good access to care for millions of people.
The escalation of these costs is a huge concern for many reasons, but it is not a uniquely American problem. Indeed, the need to lower these expenditures is shared by public and private payers in many countries, including Canada. As noted in an OECD report, “Healthcare costs are rising so fast in advanced economies that they will become unaffordable by mid-century without reforms.”
Against that backdrop, a group of researchers at the School of Public Policy at the University of Calgary studied Canada to see if a country with a publicly funded health care system could benefit from additional social spending versus health spending. Each Canadian province publicly reports spending on the health and social care systems (both of which are provincial, not federal, jurisdictions). We assembled that data from historical documents.
We took 31 years of provincial-level spending and overall budgets, demographics and macroeconomic variables – such as the unemployment rate – to build a model of how variations in spending allocations impact population health changes. Canada and the U.S. are comparable in that sub-national units (provinces and states) have jurisdiction over public health and social spending and, in both countries, the same relationship between social and health spending holds with population health outcomes.
In our study, we provide evidence that shows the ratio of social spending to health spending has an association with major population health outcomes in Canada. Important measures like life expectancy and potentially avoidable mortality appear to respond to social spending more than to health spending. Our conclusion: Governments trying to make the most of scarce resources could improve the health of their people by skewing more spending toward social services.
In Canada’s biggest province, Ontario, for example, we suggest that increasing the ratio of social-to-health spending by one cent for each dollar spent on health would have led to improvements in life expectancy of 5 percent per year and avoidable mortality of 3 percent per year. That redistribution would have been of less than 1 percent of the total health budget.
This matches state-level research from the United States. In both countries, spending on health care as a proportion of GDP is rising (in line with OECD country trends), while social spending has not seen the same increases. It is important to note that researchers – and countries – treat social spending differently. Education spending is included as social spending in the U.S. studies, but not in the Canadian. Further, other measures (ex., minimum wage legislation) might generally be considered to be part of social policy, but they are not included as such in government spending.
With or without the ACA, sub-state stakeholders in the U.S. are taking action. Hospital networks, in particular, have identified that investments in social care (e.g., housing) decrease the health care needs of their patients. Unfortunately, governments have been slower to appreciate the benefits of greater social spending; they tend to treat it as a cost, an outflow of money to solve a hopefully temporary problem. This phenomenon is known as the “wrong pockets problem.”
Researchers have suggested that an exclusive focus on health care expenditures in the discussion on how to institute reforms is misleading. Their argument, backed by comparative data from 30 industrialized countries, is that the total amount spent on both health care and social services programs explains the variance in health-related outcomes. These findings have been confirmed by additional studies using other international comparisons.
The good news is that a consensus is developing that the Social Determinants – not health care per se – are the greatest influencers of health outcomes, and most governments have begun to acknowledge that reality. The bad news is that this growing understanding hasn’t yet translated into significant policy changes on the ground. The stakes here are high. They are people’s health. Our research points to a path that Canada, the U.S. and other developed countries can follow toward a healthier future for their populations. Our hope is that they will indeed take it.
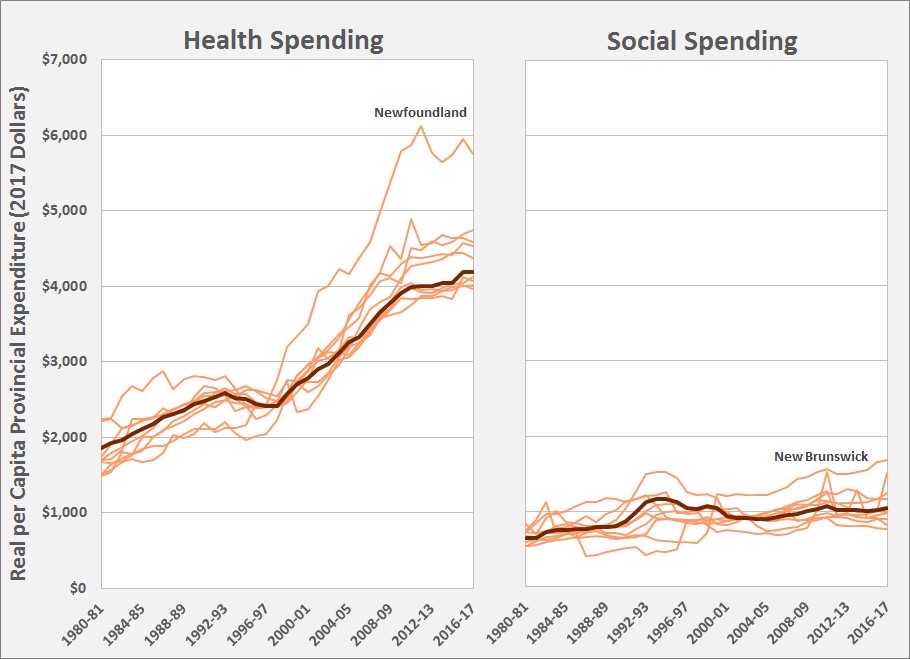
Figure: Canadian provincial spending on health and social services from 1980 to present. The dark line is the national average, the lighter lines are the individual provinces. Outliers are noted.

Figure: The alcohol harm paradox.